Stabilizing a Healthcare SaaS Platform Across 60 Hospitals.
As a Senior Product Manager with CPO-level ownership, I helped Prime eHealth stabilize its EMR and telemedicine platform, prioritize roughly 300 backlog issues, and protect hospital adoption across Nigeria.
The scale, in six numbers.
The problem was not launching features. It was keeping hospitals operational.
Prime eHealth was already serving hospitals, so the risk was not product-market fit but operational trust. Hospitals depended on the EMR for records, appointments, and clinical workflows — a failing product meant escalating support and hospitals considering leaving.
In healthcare SaaS, product debt isn't internal — it becomes hospital friction, clinical risk, and retention risk.
The EMR was already live when I joined; my focus was stabilization, backlog triage, and prioritization. The telemedicine app was the stream I shaped most directly as the patient-facing layer.
One platform, eight moving parts.
Understanding what was already live mattered before touching the backlog.
~300 backlog items across product, design, and engineering.
When I joined, the backlog spanned nine overlapping categories, none pre-sorted by urgency or risk.
The backlog triage matrix.
| Category | What It Meant | Business Risk | How I Approached It |
|---|---|---|---|
| Critical hospital blocker | Issues preventing key hospital workflows | Hospital frustration, churn risk, support escalation | Prioritized immediately with CTO/dev team |
| Technical debt | Unstable or inefficient system behavior | Slower releases, recurring bugs | Separated urgent fixes from structural work |
| Design debt | Inconsistent workflows for doctors, admins, and patients | Low adoption, training burden | Simplified flows and clarified journeys |
| Enhancement request | Hospital-requested improvements | Roadmap distraction if treated as urgent | Evaluated against impact, effort, and risk |
Critical hospital blocker
Technical debt
Design debt
Enhancement request
The inherited backlog was triaged and either cleared or brought under control within three months — through developer coordination and a weekend ticket system built to clear old issues faster.
The real blocker was not only the backlog. It was manpower.
Many open tickets, limited capacity — I requested additional frontend support, then helped onboard an intern cohort.
~4 Backend Developers
The model expanded capacity without assuming unlimited manpower.
I built a training structure with the developers so interns could catch up and support delivery.
Creating a weekend ticket system to clear old issues faster.
Normal hours covered current work. For old or urgent tickets, I proposed a weekend structure where willing developers earned extra pay per ticket resolved.
Faster Backlog Clearance
Old tickets cleared without competing with weekday delivery.
Real Incentive for Developers
Developers earned extra pay per ticket resolved.
Targeted Urgent Work
Urgent backlog got direct attention without overloading weekday delivery.
Faster Hospital-Critical Fixes
Hospital-critical issues got faster attention than the weekday queue.
How I operated with CPO-level ownership inside the product system.
I owned product prioritization and delivery coordination — running standups, assigning tasks — while partnering with the CTO on technical feasibility and system-level decisions.
Reported directly to the CEO
Translated hospital pain into backlog items
Made decisions across EMR and telemedicine
Balanced urgency with engineering capacity
Protected stability while improving the experience
The UPTH crisis: stabilizing a major hospital relationship in three days.
University of Port Harcourt Teaching Hospital (UPTH) was already using the EMR. Within my first one to two months, unresolved technical issues put the relationship at risk — losing a teaching hospital would have damaged trust, revenue, and credibility.
This was a team effort — I led the response, coordinated developers, worked with the CTO, and helped build the operating structure that resolved the issues before the CEO returned to UPTH management.
A three-day response helped stabilize a major teaching-hospital relationship.
I coordinated the response that helped retain UPTH — and UPTH stayed after the intervention.
Eight stakeholders, eight different needs.
Business continuity, hospital retention, product clarity
Clear priorities, technical feasibility, debt visibility
Clean requirements, sequenced backlog, fewer unclear requests
Reliable EMR, operational confidence, less disruption
Smoother clinical workflows, easier patient records
Easier appointments, records, and daily operations
Fewer repeated unresolved product complaints
Easier booking, telemedicine access, smoother care
Inside the operational complexity
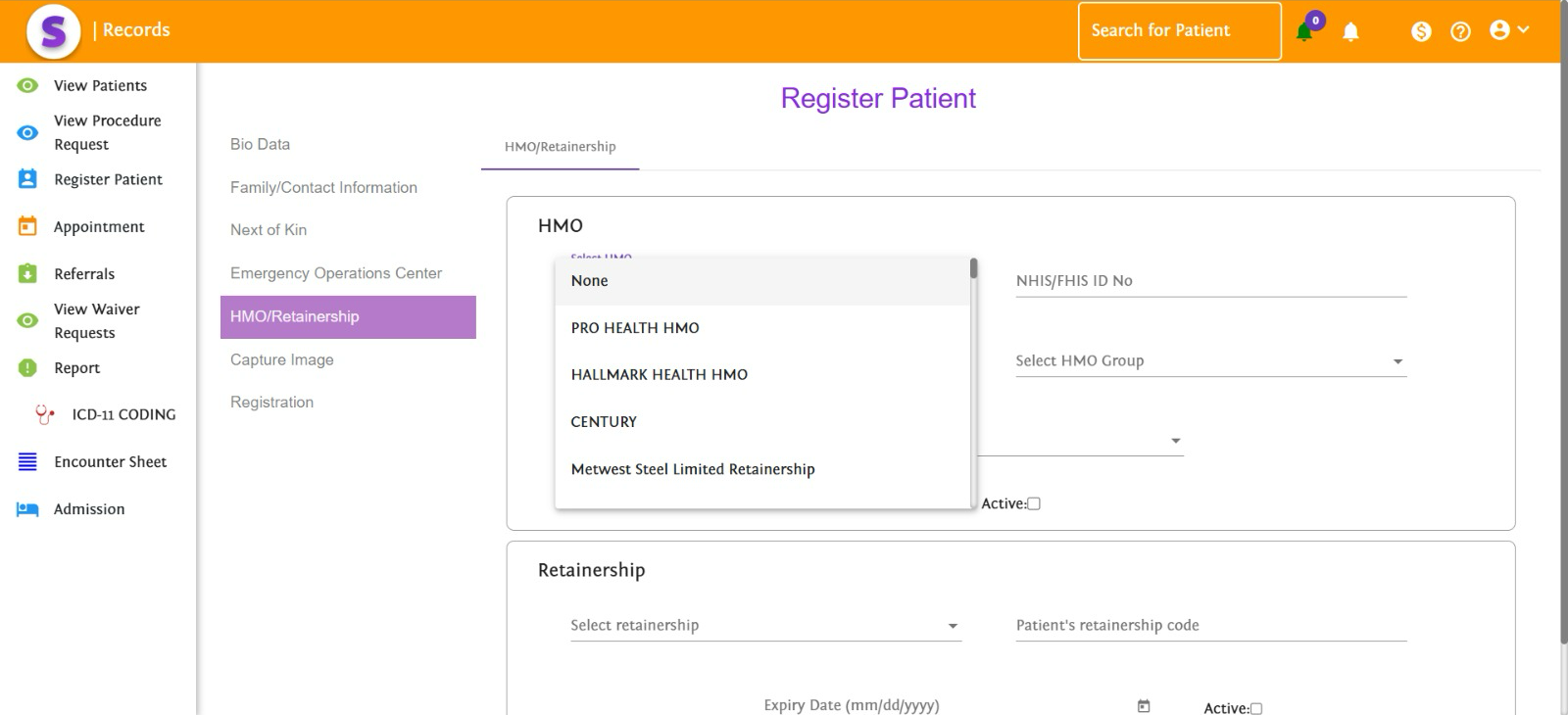
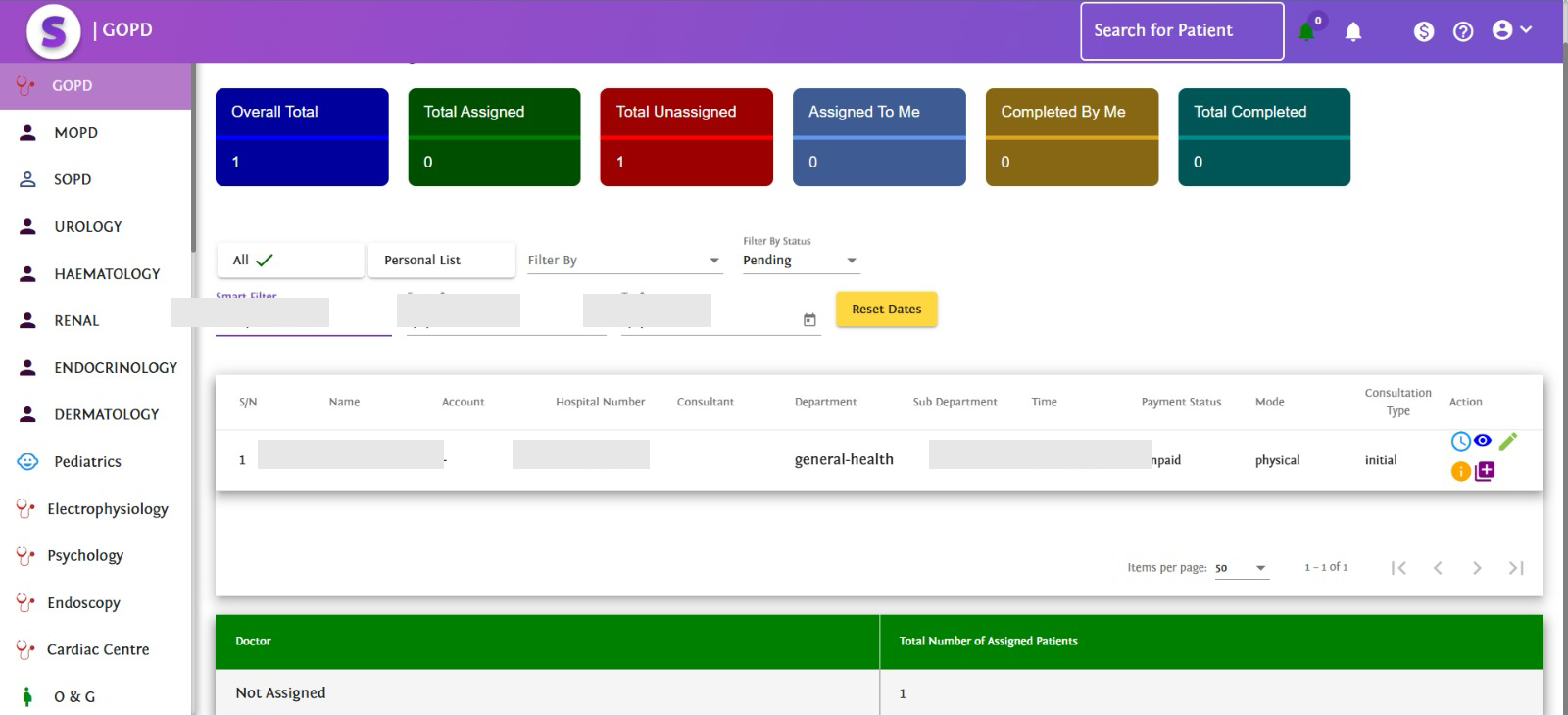
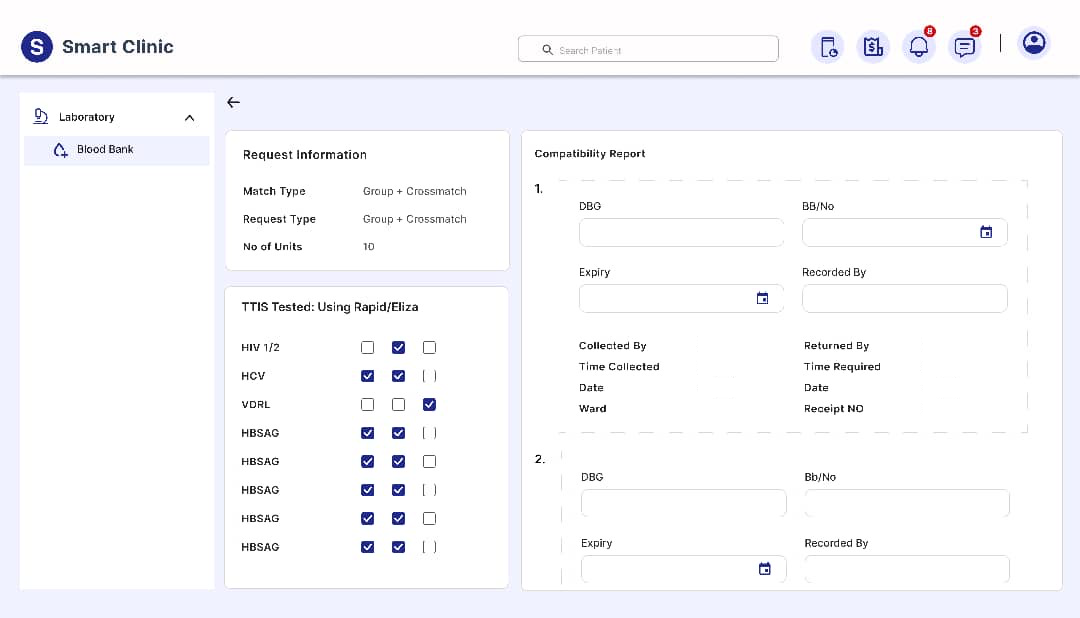
These representative views show the interconnected workflows the platform needed to support — patient registration, outpatient queues, pharmacy inventory and blood-bank operations. My responsibility was not to create the original EMR, but to stabilize its delivery system, prioritize hospital-critical failures and coordinate the teams restoring reliability.
Interface views illustrate the platform environment. Some were captured after my 2024 tenure and are not presented as exact before-and-after evidence.
Patient, staff and operational identifiers have been permanently removed to protect healthcare privacy.
Patient Registration & HMO Workflows
Patient onboarding connected records, HMO information, retainership, appointments and referrals.
Stabilizing the EMR experience for hospitals.
The work meant identifying hospital-critical blockers, separating urgent fixes from enhancements, and prioritizing workflows that affected confidence.
Workflow Reliability
Prioritized fixes protecting daily clinical and admin workflows.
Doctor & Admin Usability
Reduced friction in screens doctors and admin staff used most.
Inventory & Resource Visibility
Improved pharmacy stock and bed visibility so staff could trust the system.
Appointment & Operations
Stabilized booking and operational flows hospitals relied on daily.
Outpatient teams depended on accurate queues and completion visibility to coordinate care.
Where the EMR was breaking down.
Inventory Movement Gaps
Drugs and supplies move from a hospital's main pharmacy to outlet pharmacies; gaps created missing lines and unclear stock visibility.
Bed Availability Mismatch
The system sometimes showed no available beds when beds existed — undermining staff trust in the EMR's visibility.
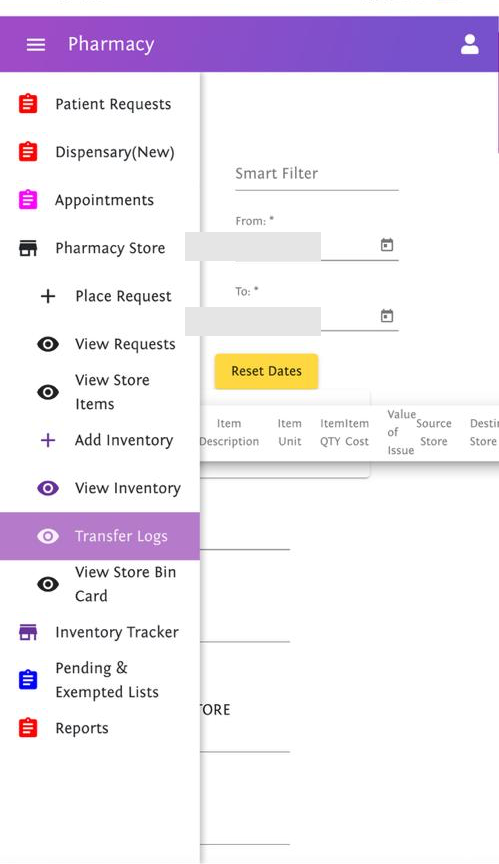
Inventory transfers between central and outlet pharmacies required dependable stock visibility and reconciliation.
In hospital SaaS, trust is operational — when staff can't trust inventory, beds, or records, the product becomes a risk rather than infrastructure.
Specialized workflows added validation, compatibility and traceability requirements where reliability was critical.
Establishing the telemedicine mobile app as the patient-facing layer.
While the EMR served hospitals internally, I helped shape the telemedicine app as Prime eHealth's patient-facing stream.
The telemedicine app had to feel simple for patients while connecting to hospital and doctor workflows.
How I decided what mattered first.
Turning backlog noise into a product roadmap.
Not every issue was urgent — here's how ~300 became a delivery system.
Capture
Every open issue in one view.
Group
Clustered into nine categories.
Rank
Scored against risk, impact, urgency.
Sequence
Ordered into a realistic delivery plan.
Align with CTO / Dev Team
Validated against real capacity.
Ship / Fix
Delivered the agreed sequence — not the loudest request.
Review Impact
Checked whether friction dropped.
How I turned crisis into an operating system.
From scattered complaints to ClickUp tickets
Issues became visible and trackable.
From limited manpower to expanded capacity
Frontend support and trained interns expanded capacity.
From fixed hours to flexible ticket resolution
Weekend paid tickets cleared issues faster.
From reactive firefighting to ranked priorities
Hospital-critical blockers were separated from normal enhancements.
From hospital frustration to restored confidence
The UPTH crisis resolved in three days, and the hospital stayed.
What changed by October 2024.
UPTH Stayed
A major teaching hospital relationship was stabilized after a three-day response.
Backlog Brought Under Control
Roughly 300 backlog items were triaged and either cleared or brought under control within three months.
ClickUp Became the Delivery System
Scattered complaints became visible, trackable, and assignable tickets.
Delivery Capacity Improved
Extra frontend support, intern onboarding, and weekend ticket work expanded the team's capacity.
EMR Trust Improved
Stabilization focused on pharmacy inventory, bed availability, and appointment-flow confidence.
Telemedicine Direction Clarified
The telemedicine app became clearer as the patient-facing layer connected to doctors and hospitals.
Executive / Technical Alignment Improved
CEO, CTO, developers, and product priorities became aligned around hospital-critical issues.
What this proves about my product leadership.
I can inherit a live SaaS product and stabilize it
I can manage product debt under business pressure
I can protect enterprise customer relationships
I can coordinate developers while working with a CTO
I can build operating systems for backlog and delivery
I can turn hospital pain into product priorities
I can balance EMR infrastructure with telemedicine growth
What I would measure next.
Because healthcare SaaS depends on trust, the next step is tracking stability, adoption, and operational confidence across hospitals.
Backlog Resolution Rate
How quickly triaged issues move to resolution.
Hospital Support Ticket Volume
Whether stabilization work reduces repeat complaints.
Hospital Retention / Churn Risk
Whether at-risk hospitals are staying engaged.
EMR Task Completion Rate
Whether core clinical/admin tasks complete without friction.
Doctor / Admin Adoption
How consistently daily users rely on the platform.
Appointment Booking Completion
Whether booking flows convert without drop-off.
Telemedicine Consultation Completion
Whether remote consultations complete end-to-end.
Time to Resolve Critical Blockers
How fast hospital-critical issues get fixed.
Release Quality / Regression Rate
Whether shipping velocity trades off stability.
Interested in how I approach product work?
Book a 20-min intro call, or send the role details by email.